
If you have been told your platelets are low during pregnancy, I know the word alone can spike your stress. Platelets are the small blood cells that help your body “seal the leaks” when you bleed. So when they drop, your mind can jump to worst case scenarios.
Here is the reassuring truth. Most low platelet counts in pregnancy are mild and harmless. But there are situations where we pay closer attention because pregnancy changes fast, and trends matter as much as numbers.
This article focuses on the two most common causes of isolated thrombocytopenia in pregnancy: gestational thrombocytopenia (GT) and immune thrombocytopenia (ITP). I will show you how doctors tell them apart, what follow up looks like, when treatment is needed, and what to watch for.
GT vs ITP
A practical clinical point: if the platelet count is below about 70,000 per µL, GT becomes less likely, and doctors actively evaluate for ITP or other causes instead of assuming it is GT.
What “low platelets” means in pregnancy
Many labs mark platelets below 150,000 per µL as low. In pregnancy, a mild decrease can happen even in healthy women. That is why one number is not enough. What matters is how low it goes, when it started, whether you have bleeding symptoms, and whether the count is stable or dropping.
If you remember one concept, make it this: your platelet trend is often more informative than a single result.
Gestational thrombocytopenia
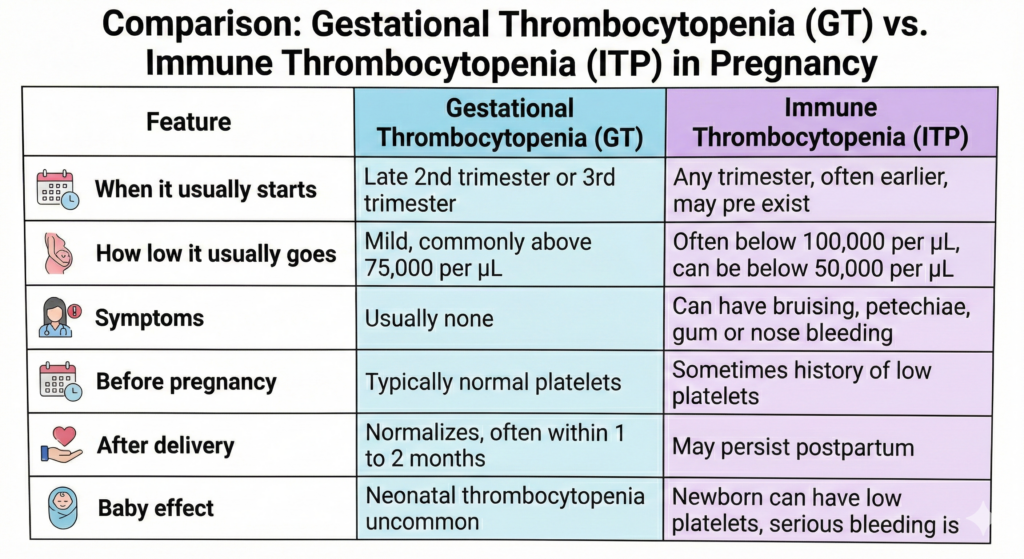
GT is the most common cause of low platelets in pregnancy. It is usually found on routine blood tests. The typical pattern is a mild drop in late pregnancy, no symptoms, and normalization after delivery.
GT does not usually cause maternal bleeding problems, and it rarely affects the baby. It also does not need treatment. The main job is monitoring and confirming that the platelets return to normal after birth.
Immune thrombocytopenia
ITP is an autoimmune condition where the immune system targets platelets and or reduces their production. It can be known before pregnancy or discovered for the first time during pregnancy.
ITP can be mild, but it can also be more significant, including counts below 50,000 per µL in some pregnancies. Symptoms can include easy bruising, petechiae (tiny red purple dots on the skin), gum bleeding, or frequent nosebleeds. Some women have no symptoms even at lower counts, which is why monitoring matters.
Unlike GT, ITP may continue after delivery.
How doctors tell GT and ITP apart
There is no single test that labels GT or ITP instantly. Doctors use pattern recognition and exclusion of other causes.
First, they confirm the platelet count is real. Sometimes platelets clump in the tube and look falsely low. A repeat CBC or a blood smear can clarify.
Second, they look at timing and previous counts. A mild drop appearing late in pregnancy with previously normal platelets strongly supports GT. A low platelet count early in pregnancy, or a known history of thrombocytopenia, raises suspicion for ITP.
Third, they make sure nothing else is going on. Conditions like preeclampsia and HELLP can also lower platelets and require urgent management. That is why your clinician may check blood pressure, urine protein, liver enzymes, and other labs if your story suggests it.
A simple way to say it: GT is the calm late pregnancy pattern. ITP is more likely when it starts earlier, goes lower, causes symptoms, or does not resolve after delivery.
Follow up in pregnancy
If the pattern fits GT and the count is mild and stable, follow up is usually light. Your obstetric team checks platelets periodically, then rechecks postpartum to confirm normalization.
If ITP is suspected, or the count is lower, or the trend is falling, monitoring becomes more structured, especially in the third trimester. This is not because something is automatically wrong. It is because we want a smooth delivery plan and to avoid last minute decisions.
If your platelet count falls below about 70,000 per µL, or if you have bleeding symptoms, hematology involvement is generally appropriate.
Treatment in pregnancy
GT
GT does not require treatment.
ITP
Many pregnant patients with ITP do not need treatment for most of pregnancy. Treatment decisions are based on bleeding symptoms, how low the platelets are, and the need to reach safe levels for delivery and anesthesia planning.
The most commonly used treatments in pregnancy are corticosteroids (often prednisone or prednisolone) and IVIG. Steroids can work well but can increase reflux, affect mood and sleep, and raise blood pressure or blood sugar in some women. IVIG can raise platelets quickly and is useful when a faster rise is needed or steroids are not tolerated.
Platelet transfusions are typically reserved for urgent situations such as active significant bleeding or urgent delivery with very low counts, often combined with other measures, because transfused platelets may not last long in ITP.
Delivery and epidural planning
This is the part that creates the most anxiety, so I prefer to make it clear early.
For delivery, many teams aim for platelets at least around 50,000 per µL. For epidural or spinal anesthesia, many teams use about 70,000 per µL as a commonly accepted threshold when there are no other bleeding risks. Decisions between 50,000 and 70,000 per µL are individualized. Below 50,000 per µL, neuraxial anesthesia is often avoided unless there are exceptional circumstances and expert agreement.
Your anesthesiologist considers more than the number. They consider your bleeding history, how stable the platelet count has been, and whether there are other lab abnormalities.
What about the baby?
In GT, the baby is usually unaffected.
In ITP, antibodies can cross the placenta, so some newborns can have low platelets. Most babies do well, but the neonatal team often checks platelets at birth, and may repeat them because the lowest point can occur in the first days after delivery. Serious bleeding in the newborn is rare, but monitoring is important.
When to seek medical care
Seek urgent assessment if you have bleeding that does not stop, heavy vaginal bleeding, blood in urine or stool, widespread rapidly increasing bruising, or new neurologic symptoms such as severe headache, vision changes, weakness, or confusion.
Also seek urgent assessment if you have symptoms that can suggest pregnancy complications that affect platelets, such as severe headache, visual changes, right upper abdominal pain, shortness of breath, chest pain, or very high blood pressure readings if you monitor at home.
If you are not sure, it is safer to be evaluated.
The five most common questions my patients ask
1) “Is this dangerous for me or my baby?”
Most of the time, no. The most common cause is GT, which is mild and resolves after delivery. If it is ITP, outcomes are usually excellent with monitoring and a delivery plan. The main risk we watch for is bleeding at very low counts, and that is exactly what follow up and treatment are designed to prevent.
2) “Is this gestational thrombocytopenia or ITP?”
GT usually appears in the third trimester and is mild, commonly staying above about 75,000 per µL. ITP can appear earlier and can be lower, including below 50,000 per µL. If the count is below about 70,000 per µL, we take a closer look and do not label it GT automatically.
3) “What symptoms should make me worry?”
Bleeding symptoms that are new or persistent matter, especially nose or gum bleeding that does not stop, heavy vaginal bleeding, blood in urine or stool, or widespread petechiae. Severe headache, vision changes, and right upper abdominal pain also matter because they can signal pregnancy complications that require urgent evaluation.
4) “Can I still have an epidural?”
Often yes. Many teams are comfortable with neuraxial anesthesia when platelets are around 70,000 per µL or higher and there are no other bleeding risks. If platelets are between 50,000 and 70,000 per µL, the decision is individualized. Planning early gives you the best chance of having options during labor.
5) “When do we treat, and what do you use?”
GT does not need treatment. In ITP, we treat if there is meaningful bleeding, if platelets become very low, or if we need to raise platelets for delivery or epidural planning. First line options in pregnancy are usually steroids and IVIG, chosen based on how quickly we need a response and what you tolerate best.
What to remember:
If you have been told your platelets are low, do not let the number steal the joy of your pregnancy. In most cases, this finding is mild and manageable, and with the right follow up it becomes a planning point, not a crisis. Ask for your trend, ask what diagnosis fits best, and make a delivery and anesthesia plan early. When you feel informed, you feel calmer, and calm helps you make good decisions.
If anything changes, new bleeding, new severe headache, vision changes, right upper abdominal pain, or a sudden drop in platelets, seek medical care promptly. It is always better to be checked and reassured than to stay home and worry.
Disclaimer
This article is for general education and does not replace medical advice, diagnosis, or treatment from your own clinician. Platelet thresholds and management decisions can vary depending on your full medical history, exam findings, pregnancy stage, other lab results, and local hospital protocols. If you have symptoms, rapidly changing platelet counts, high blood pressure, or any concern about bleeding, contact your obstetric team or seek urgent medical assessment.
References:
- ACOG Practice Bulletin No. 207: Thrombocytopenia in Pregnancy. Obstet Gynecol. 2019;133(3):e181–e193. doi:10.1097/AOG.0000000000003100.
- Bauer ME, et al. The Society for Obstetric Anesthesia and Perinatology Interdisciplinary Consensus Statement on Neuraxial Procedures in Obstetric Patients With Thrombocytopenia. Anesth Analg. 2021;132(6):1531–1544. doi:10.1213/ANE.0000000000005355.
- Matusiak K, Malinowski AK, Arnold DM. A practical approach to immune thrombocytopenia in pregnancy. Hematology Am Soc Hematol Educ Program. 2025;2025(1):503–510. doi:10.1182/hematology.2025000743.
- Fogerty AE. ITP in pregnancy: diagnostics and therapeutics in 2024. Hematology Am Soc Hematol Educ Program. 2024;2024(1):685–691. doi:10.1182/hematology.2024000595.
- Park YH. Diagnosis and management of thrombocytopenia in pregnancy. Blood Res. 2022;57(Suppl 1):79–85. doi:10.5045/br.2022.2022068.
- Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780–3817. doi:10.1182/bloodadvances.2019000812.
- Reese JA, Peck JD, Deschamps DR, et al. Platelet Counts during Pregnancy. N Engl J Med. 2018;379(1):32–43. doi:10.1056/NEJMoa1802897.
- Mangla A, Hamad H. Thrombocytopenia in Pregnancy. StatPearls (NCBI Bookshelf). Updated 2022.